











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO  uBio
uBio 
 Permalink
Permalink
INTRODUCTION
Recurrent respiratory tract infections (RRTIs) possess a relatively complex pathogenic mechanism, which involves various pathogenic factors. Children are susceptible to RRTIs, with a major age of onset of 2-6 years old, and in terms of the prevalence rate, children with RRTIs account for approximately 20.00% of children with respiratory infections 1,2. The incidence rate of RRTIs is about 16.80-18.70% in children in China, and 80.00% of children with RRTIs are aged below 5 years old 3. 25-hydroxy-vitamin D (25-OH-D) is mainly metabolized by vitamin D-25-hydroxylase. Studies have manifested that 25-OH-D is implicated in the development and progression of RRTIs, exerting a profound impact on the body immunity of developing children 4,5. Regulatory T cells (Tregs), a common subset of T cells, control the autoimmune response of the body. Animal experiments have revealed that the content of Tregs [cluster of differentiation 4 (CD4)+CD25+ Forkhead box P3 (Foxp3) Tregs] is higher in RRTI mice than that in normal mice, but it declines significantly after drug intervention 6,7. Generally, immunoglobulin E (IgE) is mainly produced in plasma cells of the respiratory and digestive tracts, which has an extremely low expression level in blood of normal people (about 0.002% of total Ig in serum), and its abnormal expression is related to the development and progression of some diseases, including RRTIs.8 Based on the above analysis, it can be concluded that there are certain correlations between expression levels of serum 25-OH-D, Tregs and total IgE and RRTIs.Kunming is situated in the Yunnan- Guizhou Plateau, China, where the incidence of RRTIs may be of specific characteristics. In addition, research on the relationship between RRTIs and expressions of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE is lacking (or rare) at present, so it is necessary to carry out such research. In this study, therefore, the expression levels and relationships of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE were explored with 150 children with pneumonia (including 53 children with RRTIs) as the subjects, aiming to provide a basis for clinical diagnosis and treatment of children with RRTIs in the plateau section.
PATIENTS AND METHODS
General data
According to the guidelines of the Declaration of Helsinki, the study was performed with approvals from the medical ethics committee of our hospital. One hundred and fifty children with pneumonia admitted to and treated in Kunming Children’s Hospital, China from January 2020 to January 2023 were selected as the subjects. The children were assigned into a control group (97 children with non-RRTIs) and an observation group (53 children with RRTIs) using a random number table.
The inclusion criteria for the observation group were set as follows: 1) children aged 0-12 years old, without gender requirement, 2) those who were diagnosed with pneumonia and met the diagnostic criteria for RRTIs, 3) those who lived in the jurisdiction of Kunming, China and 4) those whose family members and caregivers had signed the informed consent and who were willing to participate in this study. The inclusion criteria for the control group were as follows: 1) children aged 0-12 years old, without gender requirement, 2) those who were diagnosed with pneumonia and did not meet the diagnostic criteria for RRTIs, 3) those who lived in the jurisdiction of Kunming, China, and 4) those whose family members and caregivers had signed the informed consent and who were willing to participate in this study.
The exclusion criteria involved: 1) children with all kinds of congenital diseases, cancers (liver, lung, brain, pancreas, thyroid, etc.) or severe deformities, 2) those with various hematological, immunological or motor disorders, 3) those with airway obstruction, external tracheal compression, asthma, bronchiectasis or foreign bodies in the bronchus, 4) those with abnormal diet (including those with various nutritional diseases), 5) those who had taken immunosuppressants within 3 months before enrollment, 6) those with hereditary or metabolic diseases, 7) those with anemia or obesity (BMI>P95), or 8) those whose family members and caregivers were not informed or had not signed the informed consent or who had incomplete clinical data.
The control group was composed of 97 patients, including 61 (62.89%) boys and 36 (37.11%) girls, aged 0-12 (4.12±1.25) years old. As to severity of illness, there were 51 mild cases, 24 moderate cases and 22 severe cases. The observation group consisted of 53 patients, including 33 (62.26%) boys and 20 (37.74%) girls, with an age of 0-12 (4.23±1.27) years old. In terms of severity of illness, there were 27 mild cases, 16 moderate cases and 10 severe cases, respectively. As to the site of lesions, there were 34 and 19 cases of upper and lower respiratory tract infections, respectively. The general data such as age, gender and severity of illness were of no significant differences between the two groups (p>0.05), which were comparable.
Detection methods
After admission, the demographic data (age, gender, etc.) of patients were collected in both groups. The next morning, an appropriate amount (5 mL) of venous blood was collected from the elbow of each child in the company of their family members and caregivers. Then, the blood was centrifuged with a centrifuge (Beckman Coulter, USA, Optima MAX -TL) under the following conditions: centrifugal radius of 15 cm, centrifugal rate of 2000 rpm and centrifugal time of 5 min. Afterwards, the serum was harvested for measurement of 25-OH-D, CD4+CD25+CD127- Treg and total IgE expression levels. The expression level of 25-OH-D was detected by magnetic microparticle chemiluminescence assay, while the expression levels of CD4+CD25+CD127- Tregs and total IgE were measured by a flow cytometer and an automatic protein analyzer, respectively. The measurement was conducted strictly according to the specific standard operating procedures for detecting 25-OH-D, CD4+CD25+CD127- Tregs and total IgE 9.
The expressions of serum 25-OH-D, Tregs and total IgE in observation and control groups were measured and compared. Additionally, the expressions of serum 25- OH-D, CD4+CD25+CD127- Tregs and total IgE in the observation group at different stages (remission stage and attack stage), genders (boy and girl), sites of lesions (upper and lower respiratory tracts) and severities of illness (mild, moderate and severe) were measured and compared.
Statistical analysis
An Excel database was created, in which the baseline data and research data of all subjects were classified, numbered and counted. Next, such data were included in SPSS 23.0 software for processing. Count data were subjected to the χ2 test and expressed as rate or percentage (%). Measurement data were expressed by mean ± standard deviation and subjected to the t test, and analysis of variance was employed for pairwise comparison of means of three samples. The correlation was tested by Pearson analysis. Receiver operating characteristic (ROC) curves were plotted, based on which the areas under ROC curves (AUCs) were calculated to analyze the predictive values of expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE for the incidence of RRTIs. The value of AUC was between 0 and 1, where 1 represented a perfect classification and 0.5 represented random guessing. The best classification threshold was selected based on the ROC curve. At the selected optimal cutoff value, the corresponding sensitivity (true positive rate) and specificity (true negative rate) were calculated. At the selected cutoff value, the false positive rate (1-specificity) and false negative rate (1-sensitivity) were calculated. The significant level was set as α=0.05 (bilateral), and p<0.05 denoted that the difference was statistically significant.
RESULTS
Expression levels of serum 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in the two groups
The expression level of serum 25-OH-D in the observation group was significantly lower than that in the control group, whereas the expression levels of CD4+CD25+CD127- Tregs and total IgE were significantly higher than those in the control group (p<0.05) (Table 1).
Expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in children with RRTIs at different stages in the observation group
Children with RRTIs at remission stage in the observation group had a significantly lower expression level of serum 25-OH-D and significantly higher expression levels of CD4+CD25+CD127- Tregs and total IgE than those of the control group (p<0.05) (Table 2).
Table 2 Expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in children with RRTIs at different stages in the observation group.
| Stage | n | 25-OH-D (ng/mL) | CD4+CD25+CD127- Treg (%) | Total IgE (U/mL) |
|---|---|---|---|---|
| Remission | 53 | 22.31±2.25 | 4.48±1.34 | 98.67±12.33 |
| Attack | 53 | 15.64±2.17 | 6.81±1.55 | 233.61±19.55 |
| t | 15.534 | 8.279 | 42.502 | |
| p | <0.05 | <0.05 | <0.05 |
Expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in RRTI boys and girls in the observation group
In comparison with RRTI girls, RRTI boys exhibited comparable expression levels of serum 25-OH-D and CD4+CD25+CD127- Tregs (p>0.05), but a slightly elevated expression level of total IgE (p<0.05) (Table 3).
Table 3 Expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in RRTI boys and girls in the observation group.
| Gender | n | 25-OH-D (ng/mL) | CD4+CD25+CD127- Treg (%) | Total IgE (U/mL) |
|---|---|---|---|---|
| Girl | 20 | 15.57±2.26 | 6.25±1.37 | 232.51±19.82 |
| Boy | 33 | 15.82±2.23 | 6.72±1.43 | 234.57±20.59 |
| t | 0.573 | 1.728 | 2.045 | |
| p | 0.568 | 0.087 | 0.043 |
Expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in children with different severities of RRTIs in the observation group
A lower expression level of serum 25-OH-D and higher expression levels of CD4+CD25+CD127- Tregs and total IgE were detected in children with severe RRTIs compared to those in children with mild and moderate RRTIs (p<0.05) (Table 4).
Table 4 Expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in children with different severities of RRTIs in the observation group.
| Severity | n | 25-OH-D (ng/mL) | CD4+CD25+CD127- Treg (%) | Total IgE (U/mL) |
|---|---|---|---|---|
| Mild | 27 | 15.57±2.26 | 4.15±1.02 | 201.33±16.55 |
| Moderate | 16 | 15.82±2.23 | 5.84±1.23a** | 239.75±20.58a** |
| Severe | 10 | 13.08±1.85b**c* | 6.89±1.52b**c | 292.61±23.57b**c** |
| F | 5.75 | 22.99 | 84.11 | |
| p | 0.057 | 0.0000 | 0.0000 |
q test (Newman-Keuls method) for pairwise comparison of sample means (3), a: the first vs. the second, b: the first vs. the third, c: the second vs. the third. *p<0.05, **p<0.01.
Expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in children with RRTIs in the upper and lower respiratory tracts in the observation group
The expression level of serum 25-OH-D in children with RRTIs in the upper respiratory tract was significantly higher than that in the lower respiratory tract, and the expression level of total IgE was significantly lower than that in the lower respiratory tract (p<0.05) (Table 5).
Table 5 Expression levels of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE in children with RRTIs in the upper and lower respiratory tracts in the observation group.
| Site | n | 25-OH-D (ng/mL) | CD4+CD25+CD127- Treg (%) | Total IgE (U/mL) |
|---|---|---|---|---|
| Upper respiratory tract | 34 | 16.23±2.58 | 6.12±1.25 | 226.87±17.88 |
| Lower respiratory tract | 19 | 13.34±2.27 | 6.58±1.33 | 250.64±23.58 |
| t | 6.122 | 1.835 | 5.848 | |
| p | <0.05 | 0.069 | <0.05 |
Results of correlation analysis
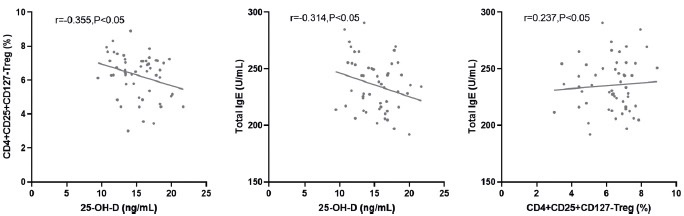
The results of Pearson correlation analysis revealed negative correlations of the expression level of serum 25-OH-D with the expression levels of CD4+CD25+CD127- Tregs and total IgE (r=-0.355, -0.314, p<0.05) and a positive correlation between expression levels of CD4+CD25+CD127- Tregs and total IgE (r=0.233, p<0.05) (Fig. 1).
Analysis results of predictive value
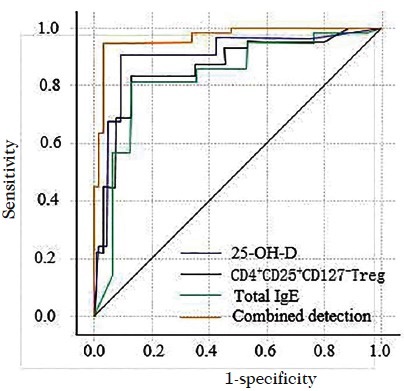
The AUC value of combination of 25-OH-D, CD4+CD25+CD127- Tregs and total IgE for predicting the incidence of RRTIs was 0.852, which was significantly larger than that of any of the three indicators alone (0.752, 0.654 and 0.643, respectively; p<0.05) (Fig. 2).
DISCUSSION
The expression level of 25-OH-D in children with RRTIs (0.5 months to 14 years old) is lower than that in healthy children (control group), and the insufficiency or deficiency of vitamin D is related to the occurrence of RRTIs 4. The lack of serum 25-(OH)-D3 in children with RRTIs is an important reason for the decreased expression level of plasma LL -37 (one of the Cathelicidin antimicrobial peptides) 10. This suggests that RRTI children have obvious vitamin D deficiency or deficit. In this study, the expression level of 25-OH-D in children with RRTIs was abnormal, which was significantly decreased compared with that in the control group (children with non-RRTIs). Such a decrease in the expression level of serum 25-OH-D may be ascribed to the following factors. Firstly, the immunomodulatory function of vitamin D is related to the expression of vitamin D receptors (in vascular endothelium, myocardium, skeletal muscle, immune cells, etc.). Vitamin D receptors have been confirmed to have no expression in resting T lymphocytes. However, when the body is infected, T lymphocytes are activated and can participate in the mediation of 25-OH-D2 by expressing cytochrome P450 family member 27B1, and make it transform into 1,25(OH) D. On this condition, the endogenous nature of vitamin D receptors is activated by stimuli, followed by combination (vitamin D and its receptors) and joint action to promote immune cells to produce corresponding cytokines, playing the role of immune regulation. As a result, body immunity is enhanced 11,12. Secondly, 25-OH-D can interact with macrophages and monocytes, producing tubulins and defensins with antibacterial and antiviral activities in the induction period, thus affecting the phagocytic ability and chemotaxis of macrophages and monocytes, and enhancing the differentiation of monocytes to macrophages 13. It follows that the decrease in the expression level of serum 25-OH-D in children with RRTIs is related to insufficient intake of vitamin D and repressed expression of vitamin D receptors.
Tregs impede the activation and proliferation of target cells inhibiting the expression of CD25 (interleukin-2 receptor subunit alpha, IL-2Ra) chain on the surface of target cells. Second, Tregs suppress the proliferation of effector cells and immunocompetence 14, i.e. Tregs secrete such inhibitory cytokines as IL-10 and transforming growth factor-β to participate in immune suppression of the body. In this study, the expression level of CD4+CD25+CD127- Tregs in children with RRTIs was subjected to a control study from the perspectives of disease stage, gender, site of lesions and severity of illness. It was found that the expression level of CD4+CD25+CD127- Tregs in children with RRTIs was abnormal, which was significantly higher than that in the control group (children with non-RRTIs), implying that the development and progression of RRTIs in children are influenced by CD4+CD25+CD127- Tregs. Schenck et al. found that the expression level of lymphocytes (CD3, CD4) in RRTI children was lower than that in the control group (healthy children) 15. Moreover, CD4+CD25+CD127- Tregs can effectively inhibit the immune response mediated by CD4+ and CD8+ effector cells16,17. This shows that CD4+CD25+CD127- Tregs exhibit abnormal proliferation and activation in RRTI children, giving rise to enhanced response advantage of Tregs, breaking the balance between T helper type 1 (Th1)/Th2/Th17 cell system and Treg cell system, and leading to the disorder of immune regulation. Eventually, RRTIs develop and progress.
In this study, the expression level of total IgE in children with RRTIs was compared from disease stage, gender, site of lesions and severity of illness. The results showed that the expression level of total IgE in children with RRTIs was abnormal and higher than that in the control group (children with non-RRTIs), signifying that the abnormal expression of total IgE is related to the development and progression of RRTIs. This is attributed to the fact that repeated respiratory infections affect the antigens, leading to the exhaustion of the immune system and increasing the expression level of total IgE in serum.
The results of Pearson correlation analysis uncovered that the expression level of serum 25-OH-D was negatively correlated with the expression levels of CD4+CD25+CD127- Tregs and total IgE (r=-0.355, -0.314), while the expression level of CD4+CD25+CD127- Tregs was positively correlated with that of total IgE (r=0.237). This demonstrates that the development and progression of RRTIs is a comprehensive pathological process, which may be caused by the interaction of serum 25-OH-D, CD4+CD25+CD127- Tregs and total IgE. It has previously been reported that the children with RRTIs (196 children aged 1 to 18 years old) had reduced serum 25-OH-D expression levels (61.00%), and vitamin D expression level was negatively correlated with age 18. In this state, the expression levels of immunoglobulins (IgA, IgG) in children with RRTIs also decrease 19. In this study, when the expression level of serum 25-OH-D in children with RRTIs dropped, that of total IgE rose, i.e., there was a negative correlation between the two. It suggests that serum 25-OH-D may be involved in mediation of humoral immunity. Beale et al. proved that the severity of RRTIs was correlated with the level of vitamin D, and in RRTI children with a low immune level, the serum 25-OH-D level showed a positive relationship with the severity of RRTIs 20. Hatam et al. confirmed that CD4+CD25+CD127- Tregs were abnormally expressed in children with RTTIs, which was an important pathogenesis of RRTIs.21 It can be concluded that serum 25- OH-D, CD4+CD25+CD127- Tregs and total IgE may participate in the development and progression of RRTIs through interaction. Moreover, it was also found in this study that the AUC value of combination of 25- OH-D, CD4+CD25+CD127- Tregs and total IgE for predicting the incidence of RRTIs was 0.852, which was larger than that of any of the three indicators alone, with significant differences. Collectively, the combined detection of the three indicators is beneficial to improving the detection rate of RRTIs.
Nevertheless, this study is limited. The obtained predictive values are focused on the analysis of global RRTIs (upper and lower respiratory tract) compared to non-RRTIs. Further studies are ongoing in our group.
In summary, serum 25-OH-D, CD4+CD25+CD127- Tregs and total IgE are abnormally expressed in children with RRTIs, and their expressions are of great differences among children at different stages, sites of lesions and severities of illness. The expression of 25-OH-D has negative correlations with the expressions of CD4+CD25+CD127- Tregs and total IgE, and a positive correlation is observed between the expressions of CD4+CD25+CD127- Tregs and total IgE. The combined detection of serum 25-OH-D, CD4+CD25+CD127- Tregs and total IgE is conducive to enhancing the detection rate of RRTIs.

