











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
Ureteral stones are a common condition of the urinary system, and their occurrence is rising worldwide. Approximately 80% of patients with ureteral stones less than 10 mm in diameter can pass them spontaneously with conservative treatment 1, but this process is often accompanied by severe pain and potential complications 2. Despite recent advances in diagnostic and therapeutic methods, pharmacological excretory therapy (MET) is increasingly recognized as an important non-surgical treatment option 3,4.
Tamsulosin, a highly selective α1A/D adrenergic receptor blocker, has been shown in several studies to reduce intraureteral pressure by relaxing the smooth muscle of the lower ureter, thereby promoting stone expulsion 5. Its mechanism of action mainly includes 6,7: (1) selectively blocking the α1D receptor on ureteral smooth muscle, reducing the frequency and amplitude of ureteral peristalsis; (2) reducing the edema of the ureteral wall; and (3) improving the urinary drainage proximal to the stone. Clinical studies have shown that tamsulosin significantly increases the rate and shortens the duration of stone expulsion from the distal ureter and reduces episodes of renal colic 8. Potassium citrate, as an alkaline drug, has multiple roles in the treatment of urinary stones 9-11: (1) increase the solubility of uric acid and cystine stones by alkalinizing the urine; (2) inhibit the formation of calcium salt crystals; and (3) replenish citrate to correct hypo-citraturia. In recent years, potassium citrate has been found to promote stone expulsion by altering stone surface charge and reducing their adhesion to the urinary tract epithelium. Some studies have shown that combination therapy is superior to monotherapy, and the rationale for combination therapy is that the two drugs may synergize to promote stone clearance through different mechanisms: tamsulosin acts primarily on ureteral dynamics, and potassium citrate may alter the physicochemical properties of the stone 12.
In clinical practice, the choice of treatment for ureteral stones requires consideration of several factors, including stone size, location, composition, symptom severity, and individual patient characteristics. In general, stones <5 mm in diameter have a high rate of spontaneous expulsion, whereas those 5-10 mm in diameter have a significantly lower rate of spontaneous expulsion13. Stone location is also an important factor influencing stone expulsion, with distal ureteral stones typically having a higher expulsion rate than proximal stones 14. In addition, stone composition, ureteral anatomical variations, and previous history of stone evacuation can affect treatment outcomes. Therefore, the search for a more effective pharmacological lithotripsy regimen is of great clinical importance. The aim of this study was to systematically evaluate the promotion effect of tamsulosin and potassium citrate alone and in combination on the spontaneous expulsion of ureteral stones, to compare the differences in stone expulsion rate, time to expulsion, and degree of pain relief, and to explore the effect of stone composition on drug efficacy, with a view to providing an evidence-based basis for the clinical development of an individualized treatment regimen. The results of the study will help optimize the conservative treatment strategy for ureteral stones, reduce patient pain, and medical costs.
MATERIALS AND METHODS
Study design and participants
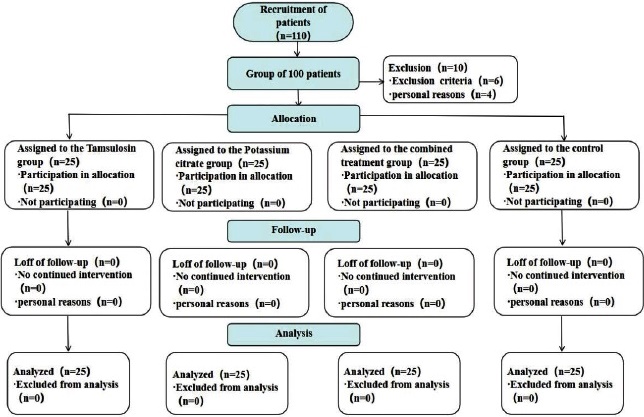
This is a clinical retrospective study aimed at evaluating the clinical effectiveness of tamsulosin therapy and potassium citrate in promoting the spontaneous passage of ureteral stones. The clinical data of patients with ureteral stones admitted to our hospital from January 2020 to December 2023 were collected, and 100 patients were ultimately included. These patients were divided into four groups based on their treatment protocols: tamsulosin group (0.4 mg/d), potassium citrate group (3 g/d), combined treatment group (tamsulosin + potassium citrate), and a control group (symptomatic treatment only). The flow chart of this study is shown in Fig. 1.
Inclusion, exclusion, and withdrawal criteria
Inclusion criteria: age 18-70 years; unilateral primary ureteral stone diagnosed by abdominal Computed Tomography (CT) scanning 15; maximum stone diameter 5-10 mm (longest diameter measured by CT) 16; receiving at least 2 weeks of standardized medication; having complete 4-week follow-up data; and a normal contralateral urinary tract.
Exclusion criteria: renal insufficiency; history of previous ureteral surgery on the affected side; pregnant women; recurrent renal colic during the follow-up period, ineffective conservative treatment, requiring surgical treatment; comorbidity with severe urinary tract infections requiring surgical treatment; and recent use of oral calcium channel blockers or alpha-1 receptor blockers.
Withdrawal criteria: exacerbation of the condition during follow-up (worsening of infection or recurrent renal colic); due to non-collection of stones (e.g., complete dissolution of stones or stone exclusion not detected); and stone composition analysis (using chemical analysis) in all patients, if the composition of the stones is non-uric acid stones.
Ethics statement
The study strictly followed the requirements of the Declaration of Helsinki and the ethical guidelines of the Wuxing District People’s Hospital of Huzhou City and was approved by this Hospital’s Ethics Committee.
Research methodology
Patients’ baseline data (age, gender, stone characteristics, etc.) were collected, and the calculus clearance achieved by 4-week follow-up was recorded. The primary observation index was the rate of stone expulsion (confirmed by ultrasound or CT), and the secondary indexes included the time of expulsion, the number of pain episodes and the adverse drug reactions. Blinded, unifactorial and multifactorial logistic regression were used to analyze the relevant factors affecting stone expulsion.
How the medication was administered: 2 packets of potassium citrate three times a day, dissolved in warm boiled water. Tamsulosin 0.2 mg/d, 1 time/d, taken orally after meals. During follow-up, each group had episodes of renal colic and was given diclofenac for pain relief. The placebo group was given diclofenac only at the onset of renal colic and no other medication. Patients in each group were asked to drink >2 L of water per day 17. The follow-up period was four weeks and was terminated if the stone was expelled within that period. Surgery was recommended for those who had not expelled the stone within four weeks.
Observation indicators
General information
Age, BMI (Body Mass Index), stone size, stone location, CT value [Hounsfield Unit (HU)], blood creatinine, uric acid, urine hydrogen ion concentration (pH), hypertension, diabetes mellitus, and the presence of hyperuricemia were recorded for the patients. A total of 110 patients met the inclusion and exclusion criteria for this trial, but 10 were excluded. The remaining 100 patients were divided into four groups based on the intervention method: 25 patients in the tamsulosin group, 25 in the potassium citrate group, 25 in the combined treatment group (tamsulosin + potassium citrate), and 25 in the control group (symptomatic treatment only).
Observation indicators
1. Recorded imaging assessment (4-week rate of complete stone expulsion)
All patients underwent low-dose unenhanced CT scans before (baseline) and after 4 weeks (±3 days) of treatment to independently assess the rate of complete stone expulsion using a blinded method.
2. Median time to stone expulsion
Confirmation of median stone expulsion time by imaging.
3. Stone location and composition
The location and composition of stones were examined using imaging and infrared spectroscopy, respectively, in each patient group.
4. Adverse reactions
Hypotension, nausea, vomiting, abdominal pain, diarrhea, and allergic reactions were recorded in each group.
5. Pain control effects
The visual analogue scale (VAS) was used to assess pain, with 0 indicating no pain and 10 representing the worst pain imaginable; higher scores indicate greater pain. The maximum reduction in VAS score was identified by noting the time when the patient first reported a significant decrease in pain and counting the number of pain episodes recorded daily, starting from the time of drug administration.
6. Imaging and laboratory indicators
The location of the stone was determined by CT before treatment, and CT was reviewed after treatment to measure the new position of the stone, calculate the three-dimensional spatial travel distance using the software Mimics Imaging, compare the average speed of stone movement (mm/ day) among different treatment groups, and record the separate distances of stone movement. Multislice spiral CT scanning was used to calculate changes in fluid volume with the software Mimics. The 24-hour urinary citrate level was recorded through sample collection.
7. Quality of life indicators
The patients were evaluated using the EuroQol 5-Dimensions 5-Levels (EQ-5D-5L) scale, which assesses mobility, self-care, daily activities, pain or discomfort, and anxiety or depression. Higher scores indicated poorer health status. The time taken to return to daily activities was also recorded, with shorter times reflecting higher patient satisfaction.
Statistical analyses
Per protocol, statistical analysis was conducted using SPSS 26.0. Efficacy endpoints (measured as mean ± SD) were analyzed with ANCOVA, adjusting for baseline values. Safety data (categorical) were compared using χ2 tests with Yates’ correction. The significance level was kept at 0.05 without applying multiplicity adjustment for this exploratory analysis.
RESULTS
Comparison of general information
A total of 110 patients met the inclusion and exclusion criteria for this trial; 10 declined to participate and were excluded. The remaining 100 patients were allocated 25 per group to the tamsulosin, potassium citrate, combined treatment, and control groups, according to the intervention modality. The demographic characteristics and baseline data of the subjects in the four groups were analyzed and were not statistically significant (p>0.05), indicating that the four groups were comparable at the pre-treatment level. As shown in Table 1.
Table 1 Comparison of patients’ general information.
| Variables | Tamsulosin group (n=25) | Potassium citrate group (n=25) | Combined treatment group (n=25) | Control group (n=25) | -/χ2/F | p |
|---|---|---|---|---|---|---|
| Age (years, mean ± SD) | 43.2±11.8 | 41.7±12.5 | 42.8±12.1 | 42.1±12.7 | 0.25 | 0.87 |
| Males (%) | 68.0 | 64.0 | 68.0 | 64.0 | 0.18 | 0.98 |
| BMI (kg/m2, mean ± SD) | 24.1±3.0 | 24.5±3.3 | 24.0±2.9 | 24.6±3.2 | 0.41 | 0.76 |
| Stone size (mm, mean ± SD) | 7.1±1.4 | 7.3±1.6 | 7.0±1.3 | 7.4±1.7 | 0.59 | 0.65 |
| Upper segment (%) | 28.0 | 24.0 | 28.0 | 24.0 | 0.21 | 0.98 |
| Mid-range (%) | 36.0 | 36.0 | 36.0 | 36.0 | 0.00 | 1.00 |
| Lower segment (%) | 36.0 | 40.0 | 36.0 | 40.0 | 0.17 | 0.98 |
| CT values (HU, mean ± SD) | 670±205 | 690±215 | 665±200 | 695±220 | 0.45 | 0.72 |
| Blood creatinine (μmol/L) | 77.8±17.5 | 79.2±18.8 | 78.0±17.9 | 79.1±19.0 | 0.16 | 0.91 |
| Uric acid (μmol/L) | 348±82 | 362±90 | 350±84 | 360±88 | 0.48 | 0.69 |
| Urine pH (mean ± SD) | 5.7±0.6 | 5.9±0.8 | 5.8±0.7 | 5.8±0.7 | 0.31 | 0.83 |
| Hypertensive | 16.0 | 12.0 | 16.0 | 16.0 | - | 1.00 |
| Diabetes | 8.0 | 12.0 | 12.0 | 12.0 | - | 1.00 |
| Hyperuricemia | 20.0 | 24.0 | 20.0 | 24.0 | 0.23 | 0.97 |
BMI: Body Mass Index, CT: Computed Tomography, HU: Hounsfield Unit, Combined treatment group: tamsulosin + potassium citrate. χ2: Chi-square Test, F: ANCOVA, -: Fisher exact. The p represents the overall difference across the four groups (Tamsulosin, Potassium citrate, Combined treatment, and Control).
Comparison of the efficacy of tamsulosin, potassium citrate and combination therapy in promoting spontaneous ureteral stone expulsion
The analysis of the effectiveness of the index in promoting spontaneous ureteral stone discharge is shown in Table 2. The stone discharge rate in the combined treatment group was optimal, with an 84.6% rate at 84.6 weeks, which was significantly higher than the rates in the single-drug groups (68.2% in the tamsulosin group and 62.1% in the potassium citrate group) and the control group (46.3%). This difference was statistically significant (p<0.001). This suggests that the combined treatment may significantly improve stone discharge efficiency through a synergistic effect (tamsulosin relaxes the ureter + potassium citrate dissolves uric acid stones). The median time to stone expulsion was shortest in the combination therapy group (6.5 days), shorter than in the monotherapy groups (9.3 days in the tamsulosin group and 11.7 days in the potassium citrate group), and significantly shorter than in the control group (14.0 days; p<0.0001). These findings indicate that the combined therapy not only enhances the expulsion rate but also accelerates the stone passage process and may reduce patients’ pain duration.
Table 2 Comparison of outcomes of patients with spontaneous ureteral stone expulsion.
| Variables | Tamsulosin Group (n=25) | Potassium citrate group (n=25) | Combined Treatment group (n=25) | Control Group (n=25) | χ2/H | p |
|---|---|---|---|---|---|---|
| 4-week stone expulsión rate (%) | 68.2 | 62.1 | 84.6 | 46.3 | 15.72 | <0.001 |
| Median discharge interval (days, 95% CI) | 9.3(8.1-10.5) | 11.7(10.2-13.2) | 6.5(5.8-7.2) | 14.0(12.5-15.5) | 28.45 | <0.0001 |
Combined treatment group: tamsulosin + potassium citrate. χ2: Chi-square Test, H: Kruskal-Wallis H. The p represents the overall difference across the four groups (Tamsulosin, Potassium citrate, Combined treatment, and Control).
Comparison of efficacy by stone location and composition
A comparison of efficacy based on stone location and composition is shown in Table 3. The lower segment stone treatment group achieved the best results, with an expulsion rate of 91.2%, which was significantly higher than the tamsulosin group (79.5%), the potassium citrate group (73.2%), and the control group (58.6%). This difference was statistically significant (p<0.001), indicating that the smooth muscle of the lower ureter is more responsive to α-blockers like tamsulosin, and that combining potassium citrate may further aid stone movement and dissolution. Upper segment stones had lower expulsion rates across all groups, with no significant difference between them (p=0.12). This suggests that upper stones are harder to expel naturally due to their anatomical position and gravity, and that medication alone has limited effectiveness. More aggressive treatments, such as extracorporeal lithotripsy, might be necessary. The expulsion rate for uric acid stones was notably higher in the potassium citrate group (78.9%) compared to the tamsulosin group (61.2%, p=0.03), and increased further to 85.4% in the combination group. This indicates that urine alkalinization with potassium citrate dissolves uric acid stones, while tamsulosin has a weaker mechanical effect on them. The clearance rate of calcium stones was higher in the tamsulosin group (70.5%) than in the potassium citrate group (55.8%), and reached 83.1% in the combined group (p<0.01). This suggests that calcium stones are resistant to dissolution and that tamsulosin helps promote their passage by relaxing the ureter, whereas potassium citrate has limited impact on them.
Table 3 Comparison of the efficacy of patients in terms of stone location and composition.
| Variables | Tamsulosin Group (n=25) | Potassium citrate group (n=25) | Combined Treatment group (n=25) | Control Group (n=25) | χ2 | p |
|---|---|---|---|---|---|---|
| Lower segment stones (%) | 79.5 | 73.2 | 91.2 | 58.6 | 18.34 | <0.001 |
| Upper segment stones (%) | 42.1 | 38.5 | 47.8 | 28.3 | 5.67 | 0.12 |
| Uric acid stones (CT<500HU) (%) | 61.2 | 78.9 | 85.4 | 42.9 | 9.12 | 0.03 |
| Calcium stones (%) | 70.5 | 55.8 | 83.1 | 47.2 | 13.45 | <0.01 |
Combined treatment group: tamsulosin + potassium citrate. χ2: Chi-square Test. The p represents the overall difference across the four groups (Tamsulosin, Potassium citrate, Combined treatment, and Control).
Analysis of safety results
The safety results are shown in Table 4, and there was no statistically significant difference in adverse reactions (p>0.05). No serious adverse reactions occurred. The combination therapy group experienced a higher rate of gastrointestinal adverse reactions, such as nausea (24%), vomiting (16%), and abdominal pain (12%), compared to other groups, indicating that the drug combination may irritate the gastro-intestinal tract. The occurrence of diarrhea was significantly higher in the potassium citrate group (16%) than in the other groups (0-8%), with the p-value reaching statistical significance (p=0.05), suggesting that potassium citrate may increase the risk of diarrhea. The incidence of hypotension was relatively higher in the tamsulosin group (12%), but there was no significant difference compared to the other groups. The rate of allergic reactions was low across all groups, indicating a favorable safety profile.
Table 4 Analysis of patient safety outcomes.
| Variables | Tamsulosin group (n=25) | Potassium citrate group (n=25) | Combined treatment group (n=25) | Control group (n=25) | χ2 | p |
|---|---|---|---|---|---|---|
| low blood pressure | 3 (12%) | 1 (4%) | 2 (8%) | 0 (0%) | 3.21 | 0.36 |
| nausea | 4 (16%) | 5 (20%) | 6 (24%) | 1 (4%) | 5.78 | 0.12 |
| vomiting | 2 (8%) | 3 (12%) | 4 (16%) | 1 (4%) | 2.94 | 0.40 |
| stomach pain | 1 (4%) | 2 (8%) | 3 (12%) | 0 (0%) | 4.15 | 0.25 |
| constipation | 0 (0%) | 4 (16%) | 2 (8%) | 0 (0%) | 7.62 | 0.05 |
| allergic reaction | 1 (4%) | 0 (0%) | 1 (4%) | 0 (0%) | 2.04 | 0.56 |
Combined treatment group: tamsulosin + potassium citrate. χ2: Chi-square Test. The p-represents the overall difference across the four groups (Tamsulosin, Potassium citrate, Combined treatment, and Control).
Assessment of pain control effectiveness
As shown in Table 5, the first pain relief time was shortest in the combination group, taking only 4.8 hours, which was significantly faster than the single-drug group (6.2 hours for tamsulosin and 7.5 hours for potassium citrate) and the control group (9.3 hours). This difference was statistically significant (p<0.01), indicating that the twodrug combination had a synergistic analgesic effect. The frequency of pain episodes was only 1.2 times per week in the combination therapy group, significantly lower tan the single-drug group (1.8 times for tamsulosin and 2.1 times for potassium citrate) and the control group (2.7 times) (p<0.05). This suggests that the combination therapy can reduce the need for analgesic medication, improve patients’ quality of life, and decrease emergency room visits. The improvement in pain intensity, measured by the VAS score, was greatest in the combination therapy group (-4.2 points), which was significantly better than the monotherapy groups (tamsulosin -3.5 points, potassium citrate -2.9 points) and the control group (-2.1 points) (p<0.001). This indicates that the combination therapy effectively reduces pain intensity.
Table 5 Comparison of patients’ pain control outcome assessment.
| Variables | Tamsulosin group (n=25) | Potassium citrate group (n=25) | Combined treatment group (n=25) | Control group (n=25) | F | p |
|---|---|---|---|---|---|---|
| Time to first pain relief (hours) | 6.2±2.1 | 7.5±2.8 | 4.8±1.7 | 9.3±3.4 | 12.36 | <0.01 |
| Number of pain episodes (times/week) | 1.8±0.9 | 2.1±1.2 | 1.2±0.6 | 2.7±1.5 | 9.54 | <0.05 |
| Maximum VAS score reduction (Δ) | -3.5±1.2 | -2.9±1.0 | -4.2±1.4 | -2.1±0.8 | 18.72 | <0.001 |
VAS: Visual Analogue Scale. Combined treatment group: tamsulosin + potassium citrate. F: ANCOVA. The p represents the overall difference across the four groups (Tamsulosin, Potassium citrate, Combined treatment, and Control).
Comparison of imaging and laboratory index assessment
A comparison of imaging and laboratory index assessments is shown in Table 6. The stone movement distance was greatest in the combined treatment group (12.3±4.1 mm), which was significantly better than that in the single-drug group (8.7±3.2 mm for tamsulosin and 6.5±2.8 mm for potassium citrate) and the control group (4.2±2.1 mm) (p<0.001). This suggests that tamsulosin can relax the smooth muscle to widen the ureter lumen, while potassium citrate reduces crystalline deposits on the stone surface; the combined treatment produces a synergistic pro-excretory effect. The improvement rate of hydronephrosis in the combined treatment group reached 78.2%, significantly higher than in the single-drug group (65.3% for tamsulosin and 58.7% for potassium citrate) and the control group (42.6%) (p<0.01). This reflects the relief of ureteral obstruction, which can prevent renal damage caused by long-term hydronephrosis. Urinary citrate excretion increased most notably in the potassium citrate and combined groups (+142±38 mg/24h and +158±42 mg/24h), significantly differing from the control group (+8±5 mg/24h) (p<0.001). Potassium citrate significantly elevated urinary citrate levels. Renal function, assessed by creatinine, improved most in the combined treatment group, with a decrease of -18.6±7.2 μmol/L, which was significantly better than the single-drug and control groups (p<0.05). This indicates the recovery of renal function after relief of obstruction, with the combination treatment providing the most comprehensive protection for renal health.
Table 6 Comparison of patients’ imaging and laboratory index assessment.
| Variables | Tamsulosin group (n=25) | Potassium citrate group (n=25) | Combined treatment group (n=25) | Control group (n=25) | χ2/F | p |
|---|---|---|---|---|---|---|
| Stone travelling distance (mm, CT) | 8.7±3.2 | 6.5±2.8 | 12.3±4.1 | 4.2±2.1 | 24.73 | <0.001 |
| Improvement rate of hydronephrosis (%) | 65.3 | 58.7 | 78.2 | 42.6 | 14.28 | <0.01 |
| 24-hour urinary citrate (mg/24h, Δ) | 25±12 | 142±38 | 158±42 | 8±5 | 32.15 | <0.001 |
| Decrease in serum creatinine (μmol/L) | -15.2±6.8 | -12.7±5.9 | -18.6±7.2 | -8.3±4.1 | 12.34 | <0.05 |
CT: Computed Tomography. Combined treatment group: tamsulosin + potassium citrate. χ2: Chi-square Test, F: ANCOVA. The p represents the overall difference across the four groups (Tamsulosin, Potassium citrate, Combined treatment, and Control).
Assessment of quality of life indicators
Quality of life indicators were evaluated as shown in Table 7, and the most notable enhancement was seen in the combined treatment group (+0.28±0.09 points), surpassing the single-drug groups (tamsulosin +0.21, potassium citrate +0.18) and the control group (+0.12) (p<0.01). This reflects overall improvement in pain management and activity levels. The quickest recovery of daily activities occurred in the combination therapy group (3.7±1.2 days), which was 30-40% shorter than the single-drug group (5.1 days for tamsulosin and 6.3 days for potassium citrate), and significantly faster than the control group (7.5 days) (p<0.001), indicating that the combination therapy increases patient satisfaction with treatment.
Table 7 Patients Comparison of quality of life indicators assessed.
| Variables | Tamsulosin Group (n=25) | Potassium citrate group (n=25) | Combined Treatment group (n=25) | Control Group (n=25) | p |
|---|---|---|---|---|---|
| EQ-5D-5L Scoring Improvement (Δ) | 0.21±0.08 | 0.18±0.07 | 0.28±0.09 | 0.12±0.05 | <0.01 |
| Resumption of daily activities (days) | 5.1±1.8 | 6.3±2.1 | 3.7±1.2 | 7.5±2.6 | <0.001 |
EQ-5D-5L: Euro Qol 5-Dimensions 5-Levels, Combined treatment group: tamsulosin + potassium citrate. F: ANCOVA. The p represents the overall difference across the four groups (Tamsulosin, Potassium citrate, Combined treatment, and Control).
DISCUSSION
Ureteral stones are a common disease of the urinary system, often leading to renal colic, urinary tract obstruction, and infection, seriously affecting the quality of life of patients 18. For stones with a small diameter (usually<10 mm), conservative treatment to promote their spontaneous expulsion is the preferred clinical strategy, but the rate of spontaneous stone expulsion is affected by factors such as stone size, location, and local inflammatory reaction in the ureter 19,20. Potassium citrate may further synergize with tamsulosin in stone expulsion rates. Therefore, the aim of this study was to systematically evaluate the efficacy and safety of tamsulosin and potassium citrate, alone or in combination, on the spontaneous excretion of ureteral stones, and to provide an evidence-based basis for optimal clinical decision-making.
Ureteral stone is a common emergency in the urinary system, this trial investigated the differences in efficacy, action characteristics and effects on different types of stones between tamsulosin and potassium citrate used alone and in combination, and systematically evaluated the differences in efficacy between these two drugs in terms of stone expulsion rate, time of expulsion, and pain control through a controlled trial. The study showed that the combination demonstrated superior efficacy compared to both mono-therapy and control groups in terms of the main efficacy indicators (p<0.01). It was further found that the combined treatment was particularly effective in lower segment stone discharge rate and uric acid stones. In terms of safety, although the rate of adverse reactions was slightly higher in the combination therapy group, it was dominated by mild dizziness and gastrointestinal reactions, and there was no significant increase in serious adverse events. The results showed that the combination of tamsulosin and potassium citrate had a synergistic effect in promoting stone expulsion, shortening the expulsion time and relieving pain, and the efficacy was significantly better than that of single-drug treatment or natural stone expulsion.
The choice of therapeutic strategy for ureteral stones requires a comprehensive consideration of stone location and compositional characteristics 21. The efficacy of pharmacological lithotripsy as an important means of non-surgical treatment varies significantly in patients with different anatomical locations and stone compositions 22. In this study, we investigated differences in the efficacy of these two drugs across patients with varying stone characteristics. The results showed that stone location and composition significantly influenced the drugs’ effectiveness: in patients with lower-segment stones, the combination therapy group had a significantly higher expulsion rate than the monotherapy and control groups (p<0.001), confirming the specific effect of tamsulosin on the lower ureteral segments; whereas, in patients with upper-segment stones, the efficacy in all groups was limited (combination group vs. control group, p=0.12), and upper-segment stones may require surgical intervention more often. Analysis of stone composition revealed that potassium citrate was significantly more effective in uric acid stones (p=0.03), while tamsulosin was more effective in calcium stones. Notably, the combination treatments consistently maintained their superiority, indicating broad-spectrum efficacy. These findings highlight the importance of personalized treatment, and clinical drug selection should consider stone location and composition.
Drug safety assessment is a crucial aspect when choosing a treatment plan 23. In pharmacological management of ureteral stones, the safety profiles of tamsulosin and potassium citrate, commonly used medications, need to be carefully evaluated 24. Tamsulosin can cause side effects such as postural hypotension and dizziness, while potassium citrate, as an alkaline agent, may lead to gastrointestinal discomfort and electrolyte imbalances 25. The present study thoroughly examined the safety profiles of these two drugs individually and in combination. Results showed that gastrointestinal side effects like nausea, vomiting, and abdominal pain were more common across all groups, likely due to the side effects of both drugs. Importantly, no serious adverse reactions were observed, suggesting a favorable safety profile for the combination therapy. These findings indicate that although the combination may increase the frequency of minor adverse reactions, it does not pose a risk of serious adverse events.
Renal colic caused by urinary stones is a common urological emergency, and rapid pain relief along with a reduction in episode frequency are essential goals of clinical treatment 26,27. In this study, the analgesic effects of different treatment options were systematically assessed by measuring the time to initial pain relief, the frequency of pain episodes, and the reduction in VAS scores. The time to first pain relief was significantly shorter in the combination group compared to the monotherapy and control groups, indicating a synergistic analgesic effect of the two drugs. The frequency of pain episodes was significantly lower in the combination treatment group than in the other groups (p<0.05), suggesting that the combination regimen not only provides quick pain relief but also effectively prevents recurrent episodes. The combination group exhibited the greatest improvement in pain levels, which was significantly higher than that of mono-therapy (p<0.001), further confirming the analgesic benefit of combination therapy. The combination of tamsulosin and potassium citrate offers notable advantages in managing pain associated with urinary tract stones, providing faster relief and more sustained reduction in both the frequency and severity of pain episodes 28.
The assessment of treatment efficacy of urinary tract stones needs to consider not only the stone expulsion rate, but also focus on comprehensive factors such as stone mobility, improvement of renal function and changes in urinary biochemical indexes 29,30. In the present investigation, we comprehensively evaluated the effects of different treatment regimens on stone kinetics and renal function using objective indicators, including stone mobility distance measured by CT, improvement in hydronephrosis, changes in 24-hour urinary citrate, and decreases in serum creatinine. Stone movement distance: the combined treatment group showed the greatest stone movement, which was significantly greater than the single-drug group (p<0.001), confirming that the combination of the two drugs synergistically enhanced stone mobility. Improvement of hydronephrosis: the highest improvement rate was observed in the combination group (p<0.01), suggesting that the combination therapy could more effectively relieve urinary tract obstruction. Change in urinary citrate: urinary citrate increased significantly in the potassium citrate and combination groups, reflecting the pharmacodynamic effect of potassium citrate. Renal function improvement: Serum creatinine decreased most significantly in the combination group, showing its advantage in protecting renal function. The study confirms that the combined treatment of tamsulosin and potassium citrate has a synergistic effect in promoting stone movement, improving hydronephrosis, and protecting renal function 31, which provides an objective basis for the clinical combined drug regimen. In particular, the combination group was significantly better than monotherapy across all indicators, suggesting that combination therapy may be a better choice for patients who require stone expulsion while improving the urinary environment and renal function.
The outcome of treatment for urinary stones requires not only objective clinical indicators, but also patient-reported outcomes (PROs) and quality of life improvement 32,33. The EQ-5D-5L, an internationally recognized quality-of-life assessment tool, provides a comprehensive picture of the patient’s health status across five dimensions: mobility, self-care, activities of daily living, pain and discomfort, and anxiety and depression 34. Meanwhile, the time to resume daily activities is an important indicator for assessing the impact of treatment on patients’ social functioning 35. This study assessed the impact of different treatment regimens on patients’ overall recovery through these two patient-centered outcome indicators. Improvement in EQ-5D-5L scores: the combination therapy group showed the greatest improvement in quality of life and demonstrated superior efficacy compared with both monotherapy and control groups (p<0.01), suggesting that combination therapy has a synergistic advantage in improving patients’ overall health status. The study results confirmed that combination therapy with tamsulosin and potassium citrate significantly improved patients’ quality of life and accelerated functional recovery. This advantage may stem from the fact that tamsulosin relieves pain symptoms faster, potassium citrate improves the urinary environment to reduce discomfort, and the synergistic effect of the two drugs shortens the overall recovery process.
In conclusion, for ureteral wall stones measuring ≤10 mm, the combination treatment was more effective than tamsulosin alone, without a significant increase in adverse drug reactions. The combination of tamsulosin and potassium citrate notably improved the stone expulsion rate for these stones and therefore warrants further clinical observation and research. Although current evidence supports the effectiveness of tamsulosin and potassium citrate in promoting spontaneous ureteral stone expulsion, this study has several limitations a lack of validation through large-scale, multicenter randomized controlled trials (RCTs), affecting the reliability of the findings. Moving forward, larger, more rigorous studies are needed, along with standardized efficacy criteria and extended follow-up periods to better establish its clinical value.

