










Servicios Personalizados
Revista
Articulo
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkArchivos Venezolanos de Farmacología y Terapéutica
versión impresa ISSN 0798-0264
AVFT v.19 n.1 Caracas ene. 2000
Dopaminergic Modulation of Human Bronchial Tone
Gloria A. Cabezas, MD; Yurina Lezama, MD; María de la Parte, MD;Freddy Contreras, MD; and Manuel Velasco MD; FRCP Edin.
Departments of Physiology, Pathophysiology and Pharmacology, "José M. Vargas" Medical School, Central University of Venezuela, Caracas, Venezuela.
ABSTRACT
Background: Dopamine exerts inhibitory and excitatory effects on different systems, independently from its adrenergic action. Its effects on bronchial tone in man have not been well studied. We examined its possible modulating effect on bronchial diameter, administering inhaled and intravenous dopamine and DA2 blockers (metociopramide) to subjects with various degrees of bronchial tone. Methods: We examined 60 volunteers. In all of them we measured arterial blood pressure and heart rate and by spirometry we measured FVC, FEV1, FEFmax and FEF50 before and after each procedure. We administered dopamine: a) through inhalation (0.5 µg/kg/min) to 10 healthy subjects, nine with asthma without acute bronchospasm (AWAB) and 18 with acute asthma attack (AAA); b) 0.5 µ/kg/min intravenous to one healthy subject and to another with AWAB. We administered intravenous metoclopramide (7 µg/kg/min) to 10 healthy subjects and 10 with AWAB. Statisfics: Studenf’s "t" test, Wilcoxon’s and Mann Whitney tests. Results: Inhaled dopamine increased FEV1 and FVC, FEFmax and FEF50 in the AAA group, but there were no modifications in the healthy group nor in the AWAB group neither by inhalation or by the intravenous route. Metoclopramide did not produce any changes of respiratory parameters in healthy individuals, nor in those with AWAB. Conclusions: 1) Inhaled dopamine produces bronchial tone inhibition when the basal tone is increased during acute asthma attack. 2) lt does not modify the basal tone in healthy individuals, nor in those with AWAB. 3) DA2 blockade does not modify basal bronchial tone neither in healthy subjects nor in those with AWAB.
Key words: human bronchial tone, airways dopamine, acute asthma.
INTRODUCTION
Airways diameter is controlled by the autonomic nervous system and by humoral pathway. Cholinergic pathways produce constriction; the adrenergic system produces dilatation through ß2 type adrenergic receptors and in some species, constriction through ð type adrenergic receptors. A non cholinergic non adrenergic inhibitory system has been described whose possible mediator in human bronchia would be nitric oxide(1). Dopamine is a precursor of adrenergic amines, but it exerts its action on peripheral tissue not only through adrenergic receptors, but also through DA1, DA2, DA3 and DA4 dopaminergic receptors(2).
The effect of dopamine over the bronchial tree is subject to controversy. Michoud et al 3) in 1984 found that inhaled and i.v. dopamine inhibited the constriction induced by the administration of successive histamine doses in healthy subjects and in subjects with asthma background. Thomson et al(4) in 1978 did not see any changes in airway conductance when administering it to healthy subjects and to those with asthma but without acute attack. Michoud(5) in 1985 observed that in vitro dopamine produced relaxation of guinea pig trachea rings and that this relaxation was blocked by propanolol (ß2 adrenergic blocker). They also found that in human and dog trachea rings, dopamine produced contraction, which was abolished by ð adrenergic receptor blockers. Kamikawa et al(6) in 1990 reported that dopamine inhibited the cholinergic and non cholinergic contraction induced by an electric field in isolated guinea pig trachea and also that the dopaminergic inhibition was not blocked by propanolol nor by yohimbine (ð adrenergic blocker), nor by haloperidol (DA2 dopaminergic blocker).
Those experiments suggested that dopamine could exert a modulating effect on airways diameter, which is manifested only when bronchial tone is increased by a cholinergic or histaminergic mechanism, or by a humoral type mechanism, as happens during an acute bronchial asthma attack.
Nevertheless, Chen(7) in 1992 found that in isolated dog trachea, dopamine produces contraction and this contraction presents tachyphylaxis, which can be restored by administering histamine to the bath, but also that this contraction restoring effect produced by histamine was partially blocked by domperidone (DA2 receptors blocker), as well as by yohimbine, but it was potentiated by atenolol (ß1 adrenergic receptors blocker).
It is evident that dopamine produces a modulating effect on airways diameter, independently from other sympaticomimetic amines, but that there are different types of responses, and correspondingly, of bronchial dopaminergic receptors, in different species. It also seems that in human airways in vitro responses are different to in vivo responses.
We decided to examine the possible in vivo modulating effect of dopamine over human airways.
OBJECTIVES
In this study we intended to examine the possible modulating effect of dopamine over airways diameter through intravenous and inhalation administration of dopamine and dopaminergic blockers to three different groups: 1) healthy persons; 2) persons with asthma but without acute bronchospasm and; 3) persons during an acute asthma attack
METHODS
Groups studied:
We studied sixty (60) persons: twenty one (21) healthy persons; twenty one (21) persons with asthma but without acute bronchospasm and eighteen (18) persons with acute asthma attack. Forty five (45) were females and fifteen (15) were males. Healthy individuals and individuals with asthma without acute bronchospasm were volunteers (medical school students and university employees). Patients with acute asthma attack were volunteers who attended the emergency service of the Vargas Hospital in search of treatment. All persons were requested to sign an informed consent form and the study was previously approved by the ethical committee of our institution.
All subjects studied were questioned regarding signs and symptoms and they were given a physical examination. All persons with a background of nervous or mental disease were excluded from the trial, as weil as those with cardiorespiratory diseases other than non complicated bronchial asthma. All pathologies were reasons for exclusion in the group of healthy volunteers.
Drug administration
Metoclopramide (MTC), a DA2 dopaminergic blocker, was used intravenously and dopamine intravenously or by inhalation. The following general scheme was followed in all cases:
Placebo1 - Experimental Drug - Placebo2
Intravenous drug administration:
Drugs were administered through Yelco Nº 20 and 22 intravenous catheters inserted into the humeral vein. The placebo solution was 5% glucose by weight, in continuous dropping during 20 minutes. Metoclopramide HCI (6 ampoules) was diluted in 5% glucose solution and administered by continuous dropping at a rate of 7µg/kg/min (dose reported in the bibliography(8) as capable of blocking DA2 dopaminergic receptors). Intravenous dopamine was administered by diluting one 50 mg/ml dopamine clorhidrate ampoule in 5% glucose solution and given with a microdrop bottle at a rate of 0.5 µg/kg/min.
Drug administration by inhalation
Hudson RCI nebulizers with nozzle were used, connected to OHIO ® flowmeters, joined to a wall oxygen outlet, with a 6 l/min flow. A 0.9% physiological saline solution was used as placebo. One 50 mg/ml dopamine clorhidrate ampoule was diluted in 0.9% physiological saline for a 0.5 µg/kg/min dose and administered by nebulizer during 20 min.
Lung function tests
Using a Fukuda model Spirosift SP 5000 spirometer, flow/volume curves obtained by Forced Vital Capacity tests were measured following the scheme suggested by the American Thoracic Society(9), before and after the administration of placebos and drugs. The following spirometric variables were analyzed: Forced Vital Capacity (FVC) in l, Forced Expiratory Volume (FEV1) in the first second in l/s, maximal Forced Expiratory Flow (FEFmax) in l/s or Peak Flow (PF) and Forced Expiratory Flow at 50% of Vital Capacity (FEF50) in l/s. All tests were carried out immediately after the corresponding nebulization or i.v.infusion.
Arterial blood pressure and cardiac frequency
Arterial systolic, mean and diastolic blood pressure and cardiac frequency were measured continuously with a CON/MED-SE 100 Dynamap. The arterial blood pressure decrease during drug administration was considered as an effect of dopamine over dopaminergic receptors.
Statistical methods
Student’s "t" parametric test, ANOVA variance analysis and Wilcoxon’s non parametric test were used, all of them for paired samples, to analyze the changes observed in the spirometric variables after placebo 1, drug and placebo 2 administration. The Mann Whitney test was used to compare among groups.
RESULTS
Intravenous dopamine
Dopamine was administered intravenously to one 21 year old healthy subject and to another 20 years old subject with asthrna background but without bronchospasm, both females. Both presented dizziness, nausea and vomit, hypotension and reflex tachycardia. In these two subjects, dopamine did not modify any of the spirometric variables as compared with controls.
Inhaled dopamine
Healthy subjects
Ten (10) subjects were studied, five (5) males with ages between 15 and 33 years (mean: 31 years), and five (5) males with ages between 23 and 40 years (mean: 32 years).
Dopamine administration did not produce significant differences in any of the spirometric variables as compared with controls. (FEV1: p>0.1; FEFmax, and FEF50: p>0.5 and FVC: p>0.1, when applying Student’s "t" test). These results indicate that inhaled dopamine does not produce changes of basal airways diameter in healthy subjects.
Subjects with asthma without acute bronchospasm
Nine (9) subjects were studied, seven (7) females with ages between 18 and 34 years (mean: 29 years), and two (2) males, 22 and 26 years old.
Dopamine did not produce significant changes in any of the spirometric variables (when using Student’s "t" test: FEV1, FEFmax, FEF50 and FVC: p>0.5). Therefore, we can conclude that inhaled dopamine does not modify basal airways tone in persons with asthma but without acute bronchospasm.
Patients with acute asthma attack
Eighteen (18) patients were studied, thirteen (13) females with ages between 14 and 32 years (mean: 21 years), and five (5) males with ages between 17 and 48 years (mean: 22 years).
When the control and placebo results for FEV1, FVC, FEF50 and FEFmax were compared, there were no significant differences (p>0.1) between placebo 1, control, and placebo 2 in any of the variables. When analyzed by Student’s "t" test and Wilcoxon’s test for paired samples, inhaled dopamine, as compared with controls, produced a statistically significant increase of FEV1 (p<0.0001), FVC (p<0.001), FEFmax (p<0.001) and FEF50 (p<0.001) (table 1). All variables increased over the 20% control value. The greatest increase seen was in FEV1 (39% of control value).
TABLE 1 Effect of inhaled dopamine in 18 patients with acute asthma attack. Comparison among spirometric parameters of controls and after dopamine administration. Statistical evaluation by Wilcoxon’s test.
| Spirometric Parameters | Control | Dopamine | Wilcoxon‘s test |
| n = 18 | X SD | X SD | p |
| FEV1 (lts) | 1 36 ± .19 | 1.90 ± .21 | .0004 |
| FVC (lts) | 1.68 ± 1.20 | 2.06 ± .99 | .0048 |
| FEFmax(lts/s) | 2.80 ± 1.43 | 3.68 ± 1.34 | .0010 |
| FEF50 (lts/s) | 1.71 ± 1.20 | 2.28 ± 1.41 | .0042 |
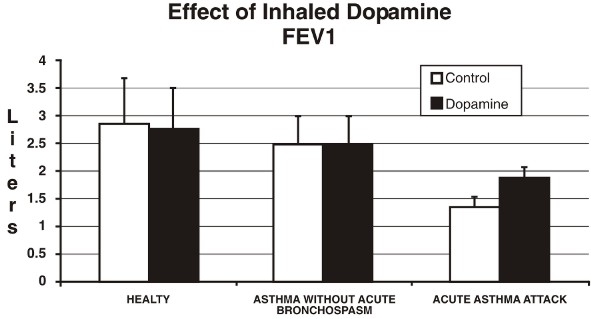
Effect of inhaled dopamine on FEV1 (Forced Expiratory Volume in the first second) in healty subjects, subjects with asthma without acute bronchospasm, and subjects with acute asthma attack; before and after dopamine inhalation. The results are expresed as Mean ± SD.
Comparison among groups which received inhaled dopamine
Figure 1 shows the FEV1 changes observed in the three groups: healthy, with asthma without acute bronchospam, and those undergoing an acute asthma attack.
Using the Mann Whitney test, we compared the effect of inhaled dopamine over FEV1 in the three groups. The difference between healthy subjects and patients with asthma but not acute bronchospasm was not significant (p= 0.1042); the difference between healthy subjects and patients with acute asthma attack was highly significant (p= 0.001), as well as the difference between patients with acute asthma attack and those who only had an asthma background but not acute bronchospasm. (p= 0.0001).
'Intravenous metoclopramide (MTC)
Healthy subsects
Ten (10) persons were studied, seven (7) females with ages between 19 and 22 years (mean: 20 years), and three (3) males, 18, 24 and 29 years old.
MTC administration did not produce any significant change in the spirometric variables studied. Using Student’s "t" test, FEV1, FEFmax, FEF50 gave a p>0.8, and FVC gave p>0.1, indicating that MTC does not modify basal airways diameter in healthy subjects.
Subjects with asthma but without acute bronchospasm
Eleven (11) female subjects were studied with ages between 20 and 40 years (mean: 23 years).
Neither in this group did MTC administration produce significant changes in the variables studied. Using Student’s "t" test, FEV1 and FEFmax gave p>0.1; FVC, p>0.5; and FEF, p0.01. This shows that MTC does not modify basal airways diameter in persons with asthma but without acute bronchospasm.
DISCUSSION
Dopamine administered by inhalation produced bronchodilation in patients suffering from acute asthma attack and this bronchodilation is important from a therapy point of view since FEV1 increased with dopamine up to 39% of the control value, and all the other variables which indicate increase of respiratory flow reached a higher than 20% increase. These results are consistent with those observed by Michoud et al(3) in persons with asthma background in whom they induced constriction with histamine. We did not observe any modifications of bronchial tone in healthy persons, or in patients with asthma but without acute bronchospasm at the moment of the study. Therefore, we can state that dopamine exerts its inhibitory effect only when bronchial tone is increased. This could explain the lack of response seen by Thomson(4) and Michoud(5) in healthy and with asthma background subjects when they administered dopamine by inhalation and intravenously without previously increasing bronchial tone. We cannot rule out an indirect effect of dopamine through the release of chemical mediators in bronchial asthma.
There were no significant differences between control and placebo 2, administered 30 minutes after dopamine, indicating that the inhibitory effect of dopamine is of short duration. This short duration of the dopaminergic effect could be due to the low doses administered, or rather to a rapid dopamine metabolism in the lung. Sumikawa et al(10), in 1991, administering various dopamine doses to humans and measuring pulmonary plasma dopamine concentration and total plasma dopamine concentration, found that dopamine was cleared up to 21% in human lungs.
The dopamine doses administered by inhalation produced decrease in blood pressure, indicating that the blood level reached is that of activation of dopaminergic receptors which inhibit arterial blood pressure (dopaminergic dose) reported by Goldberg and Rajfer(11) in 1985 and by Martin et al(12) in 1993, mediated by DA1 receptors.
Intravenous dopamine administration did not produce any effect on the spirometric variables studied in one healthy person nor in another with asthma background; the doses administered were low (dopaminergic dose) but capable of producing systemic alterations. It is possible that a fast dopamine degradation in tissues and in the pulmonary vascular bed could have prevented the observation of its effect at a bronchial level.
Dopamine administered by inhalation could exert its inhibitory action on bronchial muscular tone stimulating DA2 type receptors. Therefore, blockade of these receptors would produce an increase of bronchial tone in healthy persons and in those with the bronchial hyperreactivity characteristic of patients with asthma background. In the present paper, we did not obtain any evidence of basal bronchial tone modifications in subjects belonging to both of the above groups after administering MTC intravenously. For ethical reasons we did not administer MTC to the group of patients with acute asthma attack. These results suggest that the bronchodilating effect of dopamine would not be mediated by DA2 type receptors. More research in this field is needed.
REFERENCES
1. Barnes PJ. What is the role of nerves in chronic asthma and symptoms?. Am J Respir Crit Care Med. 1996; 153: S5-S8. [ Links ]
2. Velasco M, and Luchsinger A. Dopamine: Pharmacological and Therapeutic aspects. Amer J Therap. 1998; 5: 37-43. [ Links ]
3. Michoud MC, Amyot R, Jeanneret - Grosjean A. Dopamine effect on Bronchomotor tone in vivo. Am Rey Respir Dis 1984; 130: 755-758. [ Links ]
4. Thomson NC, Patel KR. Effect of dopamine on airways conductance in normal and extrinsic asthmatics Br J Pharmacol. 1978; 5: 421-424. [ Links ]
5. Michoud MC, Amyot R, S-JeanS. Vaillancourt R. The effect of dopamine on tracheal smooth muscle. Clin Exp Pharmacol Physiol. 1985; 12: 51-59. [ Links ]
6. Kamikawa Y, Shimo Y. Inhibitory effects of catecholamines on cholinergically and non cholinergically mediated contractions of guinea-pig J Pharm Pharmacol. 1990; 41: 131-134. [ Links ]
7. Chen CJ, Shue CH. Effect of histamine treatment on dopamine tachyphylaxis of canine tracheal smooth muscle. Respiration. 1992; 59: 107-11. [ Links ]
8. Blanco M, Jelambi I, Pérez G, Gómez J, Franco T, Hurtado N, Velasco M. The effect of intravenous metociopramide on blood pressure in normotensive and hypertensive subjects. J Clin Pharmacol Ther 1996; 34: 390-392. [ Links ]
9. American Thoracic Society. Standarization of spirometry : 1987 update Am Rev Respir Dis. 1987; 136: 1285-1298. [ Links ]
10. Sumikawa K, Hayashi Y, Yamatodani A, Yoshiva I: Contribution of the lungs to the clearence of exogenous dopamine in humans. Anest Analg. 1991; 72: 622-626. [ Links ]
11. Goldberg, LI, Rajfer EI. Dopamine receptors: application in clinical cardiology. Circulation. 1985; 72: 245-248. [ Links ]
12. Martin F, Forte P, Luchsinger A, Mendoza F, Urbina-Quintana A, Hernández Pieretti O, Romero E, Velasco M. Effect of intravenous dopamine on blood pressure and plasma insulin in hypertensive patients. Europ J Clin Pharmacol. 1993; 45: 503-505. [ Links ]

{kind=link}